










The National Cardiogenic Shock Initiative (NCSI) was assembled to assess the impact of early mechanical circulatory support (MCS) in patients with acute MI (AMI) and cardiogenic shock (CS) treated with percutaneous coronary intervention (PCI). Before establishment of the NCSI in 2016, there was significant variability in the use of MCS in AMI-CS. There were no standardised practices, and outcomes associated with the use of MCS in AMI-CS were variable. In addition, experience in the use of large-bore MCS placement, management and approval was only beginning to grow. There were also limited data on the association of right heart failure, intensive care unit (ICU) management of MCS, MCS weaning and escalation.
The NCSI addressed these needs by providing a uniform shock protocol to help healthcare systems obtain predictable outcomes and a set of standardised best practices based on foundational principles. The initiative offers a number of protocols to improve patient survival by encouraging the early use of Impella pre-PCI during optimal PCI techniques of the target artery or other large-bore vessels and avoiding escalating vasopressor and inotrope doses, which are associated with poorer outcomes. The initiative enables devices to be weaned based on invasive haemodynamics with right-sided heart catheterisation and offers hub-and-spoke models of care for the transfer of patients. Overall, the NCSI has consistently demonstrated survival in AMI-CS of over 70%.1
Over the past few years, the NCSI has continued to collect data to improve its best practice protocols on the mechanical support management of these patients with AMI. This has included data from the Cardiogenic Shock Working Group on the use of invasive haemodynamics in guiding therapy, a practice that has been shown to improve survival in AMI-CS.2 Conversely, a delay in treatment and delivery of MCS is associated with higher mortality in AMI-CS.3 This finding is consistent with evidence that CS should be treated acutely and with minimum delay to reverse the CS state.
The Impella device can also help predict right-sided heart failure. Evidence obtained by the NCSI has shown that of the 92% of patients with right ventricular (RV) catheterisation, those who had RV failure (RVF) had an absolute mortality of approximately 14% more than those without RVF.4 However, despite these favourable outcomes, the NCSI found that the use of RV haemodynamic support devices for treatment escalation is <20% in practice.4 Similarly, instead of escalating treatment to mechanical support devices, patients in AMI-CS are often maintained on increasing doses of vasopressors and inotropes, which are associated with increased mortality independent of underlying cardiac power output.5,6 NCSI analysis found that the cause of death for the majority of patients is due to ongoing CS (58%) and multiorgan failure (18%), but only 19% of patients in CS receive escalation of treatment appropriate for worsening CS.2,3 The NCSI also found that there was a considerable variation in ICU-level care and the ability of sites to escalate MCS.2 Unless sites have the appropriate tools and devices, they are unable to effectively treat patients in CS with haemodynamic support and improve clinical outcomes.
Taking all the learnings from the NSCI, Dr Basir and his team designed the study Can Escalation Reduce Acute Myocardial Infarction in Cardiogenic Shock (CERAMICS). Twenty sites were selected, all with rapid MCS escalation capabilities, including Impella, RV MCS and ECPella support devices. Data were collected on the survival of all AMI-CS patients, including those not treated with Impella.
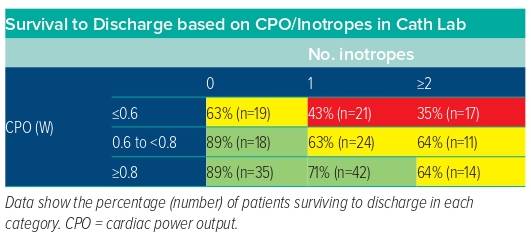
The sites participating in the trial used the same definitions as per the NCSI protocol, namely Society for Cardiovascular Angiography and Interventions (SCAI) SHOCK classes C, D and E. AMI was defined as ischaemic symptoms with ECG and/or biomarker evidence of ST-elevation MI (STEMI) or non-STEMI. CS was defined as at least two of the following: hypotension (systolic blood pressure [SBP] <90 mmHg or the use of inotropes or vasopressors to maintain SBP); signs of end organ hypoperfusion, including cool extremities, oliguria/anuria, elevated lactate concentrations, altered mentation; and hypodynamic evidence of hypoperfusion, represented by a cardiac index <2.2 l/min/m2 or cardiac power output <0.6 W. The NCSI protocol was adhered to, which includes escalation of treatment with quick implantation of the Impella CP, followed by revascularisation and right heart catheterisation for monitoring to rapidly reduce the use of inotropes. Escalation could occur at any time, but ideally as early as possible and preferably in the cardiac cath lab. Key triggers for escalation with an unloading strategy were guided by haemodynamics and aimed at achieving survival >80% (Table 1). The implementation of shock protocols alongside a team-based approach is associated with improved patient outcomes.
Dr Basir closed his presentation by confirming that the foundations, strategy and principles of the NSCI will be studied further in the CERAMICS study, as well as in the RECOVER IV randomised controlled trial for AMI-CS patients.