









Dr Frederiksen’s research examined the effect of the Impella RP and vasoactive treatment on left ventricular (LV) longitudinal strain during cardiogenic shock.
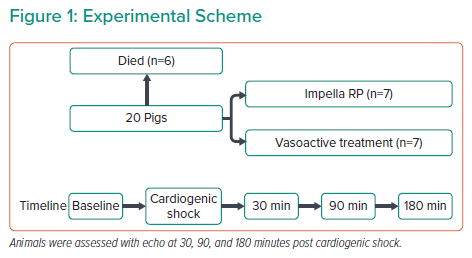
Dr Frederiksen used a porcine model of cardiogenic shock with right coronary artery embolisation, where shock was defined as a ≥50% reduction of cardiac output and/or a ≥50% reduction of venous oxygen saturation (SvO2) compared with baseline or an absolute SvO2 of <30%. The interventions used in the study included Impella RP or vasoactive treatment with milrinone and norepinephrine. The Impella RP was kept at the highest performance level throughout the entire study period, and the vasoactive treatment was initiated with norepinephrine for 30 minutes, and then an initial dose of milrinone followed by continuous infusion. For each intervention, seven animals were examined with echocardiograms obtained at five time points: baseline, cardiogenic shock and after 30, 90 and 180 minutes of treatment (Figure 1). Obtaining high-quality echocardiogram images required making a subxiphoid incision to allow the probe to be directly placed at the diaphragm. Haemodynamic data were also collected with conductance catheters (to measure ventricular volume based on blood electrical conductance) in both the LV and right ventricle, and Swan-Ganz catheters in the pulmonary artery. Blood gas analysis was performed on samples collected from the jugular vein, renal vein, arterial line and pulmonary artery.
Comparisons of echocardiograms revealed that cardiogenic shock severely reduced longitudinal function of the right ventricle. The septum lost nearly all function, and paradoxical movement was observed when the hyperdynamic lateral wall was contracting. Previous work focusing on the right ventricle showed a large reduction in SvO2 when in shock.1 However, implementation of the Impella resulted in increased SvO2 and reduced myocardial work, whereas vasoactive treatment increased SvO2 but at the cost of increased myocardial work. Dr Frederiksen and colleagues focused their analysis on the LV, which was divided into septal and lateral walls.
Dr Frederiksen presented LV strain results from speckle-tracking echocardiography, which produces a negative percentage as a readout; more negative strain values indicate a higher hyperdynamic state, whereas less negative strain values indicate reduced cardiac function. Dr Frederiksen noted how shock induction led to a decline in LV function from baseline, with less negative strain. Both treatments resulted in an improvement in overall strain values. Examination of the septal wall showed no changes from either treatment once in cardiogenic shock; conversely, the lateral wall was greatly affected by both treatments, with vasoactive treatment resulting in more negative strain than baseline over time and the Impella RP treatment resulting in normalisation to baseline values. The lower overall strain with vasoactive treatment suggests greater improvement in LV contractile function; however, it also suggests a higher energy consumption, undesirable in stress conditions. Therefore, in the context of MI shock, the lower-than-baseline strain under vasoactive treatment is not ideal for the heart.
Dr Frederiksen concluded that under profound cardiogenic shock due to occlusion of the right coronary artery, LV strain is immediately impacted. Both Impella RP and vasoactive treatment improved lateral wall strain, whereas vasoactive treatment produced greater negative strain, signalling increased energy consumption.