










Increasing age is an important risk factor for acute coronary syndrome (ACS). Population ageing means that the prevalence of ACS, and non-ST elevation acute coronary syndrome (NSTEACS) in particular, is rising.1,2 However, the evidence base to guide the optimal management of older people with NSTEACS is limited, particularly if they have concomitant frailty.3,4 Frailty describes a state of increased vulnerability to poor resolution after a stressor and is common in older adults with NSTEACS.5,6
In general, older people less frequently receive guideline-recommended management, including coronary angiography, following NSTEACS than younger patients. This variation in care may reflect uncertainties in both the evidence to support an invasive approach in this population and international guideline recommendations.7–12
Previous data have shown that frailty is a better predictor of adverse outcomes following ACS than chronological age alone.13–15 Yet, we lack data on the association between frailty, coronary angiography features and clinical outcomes in older patients with NSTEACS; these data are needed to support decision-making in this population. Therefore, in the present prospective cohort study we evaluated the angiographic and procedural characteristics in older adults with NSTEACS by frailty category. We also evaluated the association of baseline and residual SYNTAX scores with long-term major adverse cardiovascular events (MACE).
Methods
Setting and Participants
This is a prespecified subgroup analysis of the study to Improve Cardiovascular Outcomes in high-risk patients with acute coronary syndrome (ICON1). The full study design has been published elsewhere.16 The ICON1 study was a multicentre prospective cohort study of patients aged ≥75 years with NSTEACS referred for invasive coronary angiography to either Freeman Hospital, Newcastle, UK (receiving patients referred from six district hospitals) or James Cook University Hospital, Middlesbrough, UK (receiving patients referred from five district hospitals). Patients were recruited between November 2012 and December 2015.16 All patients underwent coronary angiography and guideline-recommended management of NSTEACS, in accordance with current European Society of Cardiology guidelines.3
The study received ethics approval from the National Research Ethics Service (12/NE/0160). Participants provided written informed consent, and the study was conducted in accordance with the Declaration of Helsinki.
Variables and Data Sources
Participants were evaluated for frailty at the time of admission by the research team using the Fried criteria, which consist of subjective and objective assessments of slowness, weakness, low physical activity, exhaustion and weight loss.17 Patients were considered robust if no criteria were met, prefrail if one or two criteria were met and frail if three or more criteria were met.
Baseline data were collected during the index presentation and are reported by frailty category. The data collected included population demographics (age and sex), clinical characteristics (BMI, smoking status, Global Risk of Acute Coronary Event 2.0 score, New York Heart Association [NYHA] grade, Canadian Cardiovascular Society Angina Score), frailty (according to Fried criteria), comorbidity (according to the Charlson comorbidity index), past medical history, laboratory tests at admission and baseline medical history (antithrombotic medication, statins, angiotensin-converting enzyme inhibitor or angiotensin receptor blocker, β-blocker, calcium channel blocker, anticoagulant medication).
Procedural data included femoral or radial access, the use of a glycoprotein IIb/IIIa inhibitor or unfractionated heparin, contrast volume, radiation dose and duration of procedure. Angiographic characteristics included vessel dominance, number of diseased vessels and number of lesions. Percutaneous coronary intervention (PCI)-related data were collected (i.e. number of treated vessels, complexity of the PCI procedure [rotablation or laser], number of stents and stent type). The SYNTAX score was calculated according to standard SYNTAX score criteria (www.syntaxscore.org).18
Angiographic data were analysed using QAngio XA Medis in a core laboratory at Newcastle University by at least two independent researchers, blinded to all other data. Angiographic quantitative and qualitative data were reported for the culprit lesion and were stratified by frailty phenotype. Quantitative angiographic analysis was performed on the angiographic frame with maximal stenosis, with hand-drawn contours around the lumen diameter and the lumen diameter and lesion length at the site of each diseased vessel. The analyses were conducted according to standard criteria using previous definitions and included: culprit artery, culprit vessel quantitative analysis (lesion diameter stenosis, length, vessel diameter, lesion area, minimum lumen diameter) and culprit qualitative analysis (calcification grade, eccentric, diffuse ostial or bifurcation lesion, ulcer, pulsatile or slow flow, collaterals and collateral score [0–3], thrombus and thrombus score [0–5], and lesion complexity [Type A, Type B1, Type B2 or Type C]).19–22 For patients undergoing PCI for a culprit lesion, SYNTAX scores were calculated before and after PCI (baseline and residual SYNTAX score, respectively) and stratified by frailty phenotype. Baseline SYNTAX scores were classified as low (0–22), moderate (23–32) and high (≥33), whereas residual SYNTAX scores were divided into three groups according to clinical relevance: ‘complete revascularisation’ (0), ‘acceptable incomplete revascularisation’ (1–7) and ‘unacceptable incomplete revascularisation’ (≥8).23
Five-year follow-up data were collected from electronic primary and secondary care patient records, linked to National Health Service (NHS) Digital. MACE was a composite of all-cause mortality, MI, stroke or transient ischaemic attack, repeat unplanned revascularisation and significant bleeding (defined as Bleeding Academic Research Consortium [BARC] Type 2 or greater).16
Statistical Analysis
Baseline characteristics, procedural and angiographic features and culprit lesion quantitative and qualitative angiographic analyses are reported by frailty phenotype. Categorical data are presented as numbers and percentages and were compared using the Chi-squared (χ2) test or Fisher’s exact test. Continuous variables were tested for normal distribution using the Kolmogorov–Smirnov test, with normality defined as p>0.05. Variables that were not normally distributed had a Q-Q plot drawn and inspected. Normally distributed variables are presented as the mean ± SD and were compared using independent samples t-tests. Non-normally distributed variables are presented as the median and interquartile range (IQR) and were compared using the Kruskal–Wallis one-way test of variance.
Paired student’s t-tests were used to analyse the mean difference in quantitative angiographic variables measured in the culprit artery before and after PCI stratified by frailty phenotype.
Logistic regression was used to model the association between frailty and baseline and residual SYNTAX scores, presented as unadjusted ORs with 95% CIs. Two adjusted logistic regression models were constructed: one model adjusted for age and sex, and the second model adjusted for baseline characteristics that differed between frailty groups at baseline (age, sex, previous MI, previous transient ischaemic attack or stroke, heart failure, anaemia).
To evaluate whether procedural success modifies the relationship in clinical outcomes in this older cohort in terms of composite endpoint in 5-year follow-up, Cox proportional hazards models were used with residual SYNTAX score included. Unadjusted HRs with 95% CI are reported, alongside those adjusted for age and sex.
All analyses were performed using SPSS Statistics version 27 (IBM Corporation), with significance set at p≤0.05 (Supplementary Material Table 5).
Results
Baseline Characteristics
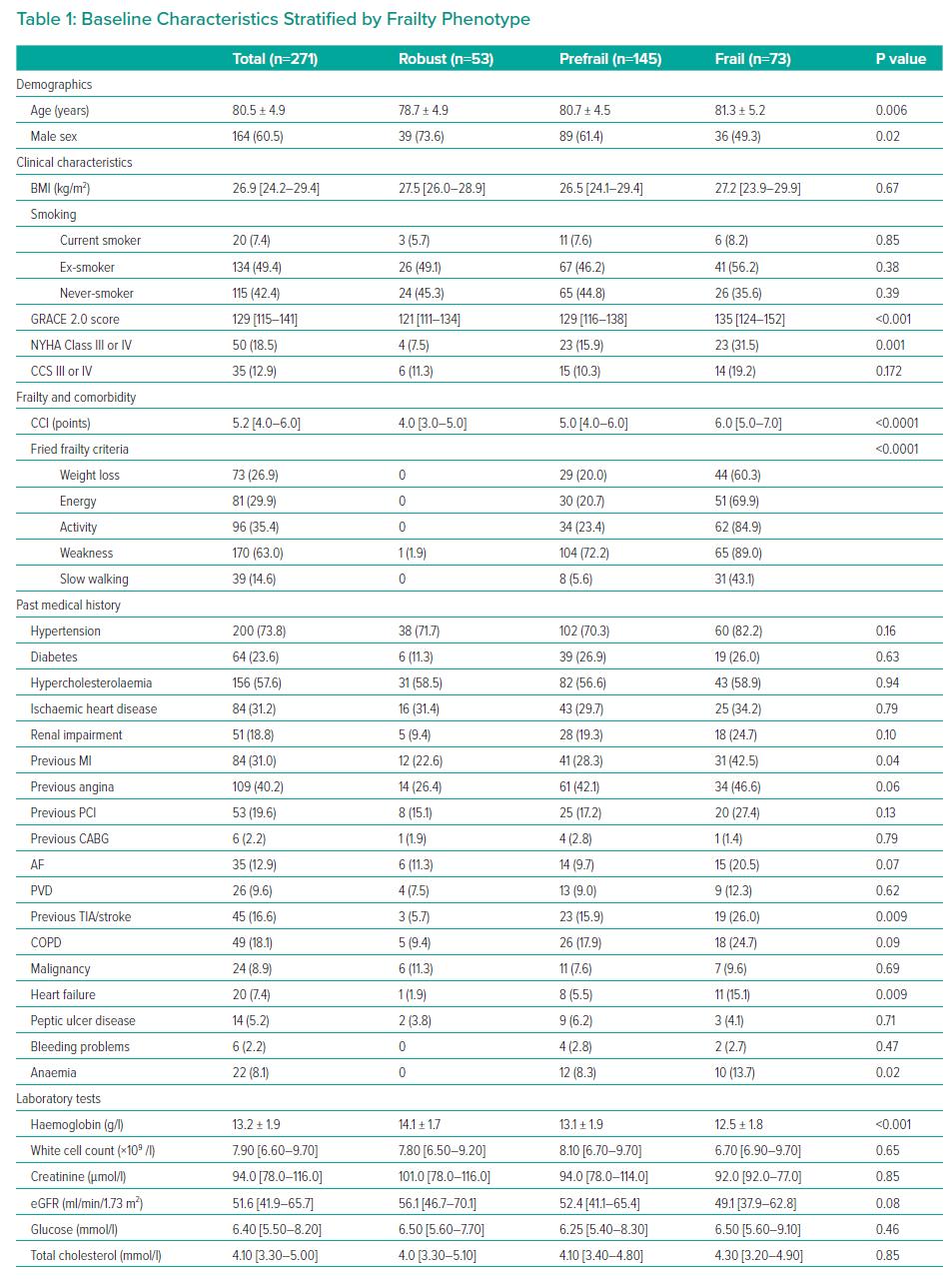
The ICON1 study cohort comprised 297 patients; the 271 (91.2%) patients for whom angiographic data were available were included in the present substudy (Supplementary Material Figure 1). Of these 271 patients, 53 (19.6%) were robust, 145 (53.5%) were prefrail and 73 (26.9%) were frail. Mean age increased with increasing frailty (78.7 ± 4.9, 80.7 ± 4.5 and 81.3 ± 5.2 years for the robust, prefrail and frail groups, respectively), with a decreasing proportion of males with increasing frailty (n=39 [73.6%], n=89 [61.4%] and n=36 [49.3%] in the robust, prefrail and frail groups, respectively). Robust patients were less often admitted with a NYHA class of III or IV (n=4 [7.5%], n=23 [15.9%] and n=50 [31.5%] in the robust, prefrail and frail groups, respectively; p=0.001; Table 1). There were no differences in medications among frailty phenotypes (Supplementary Material Table 1).
Baseline Angiographic Analysis
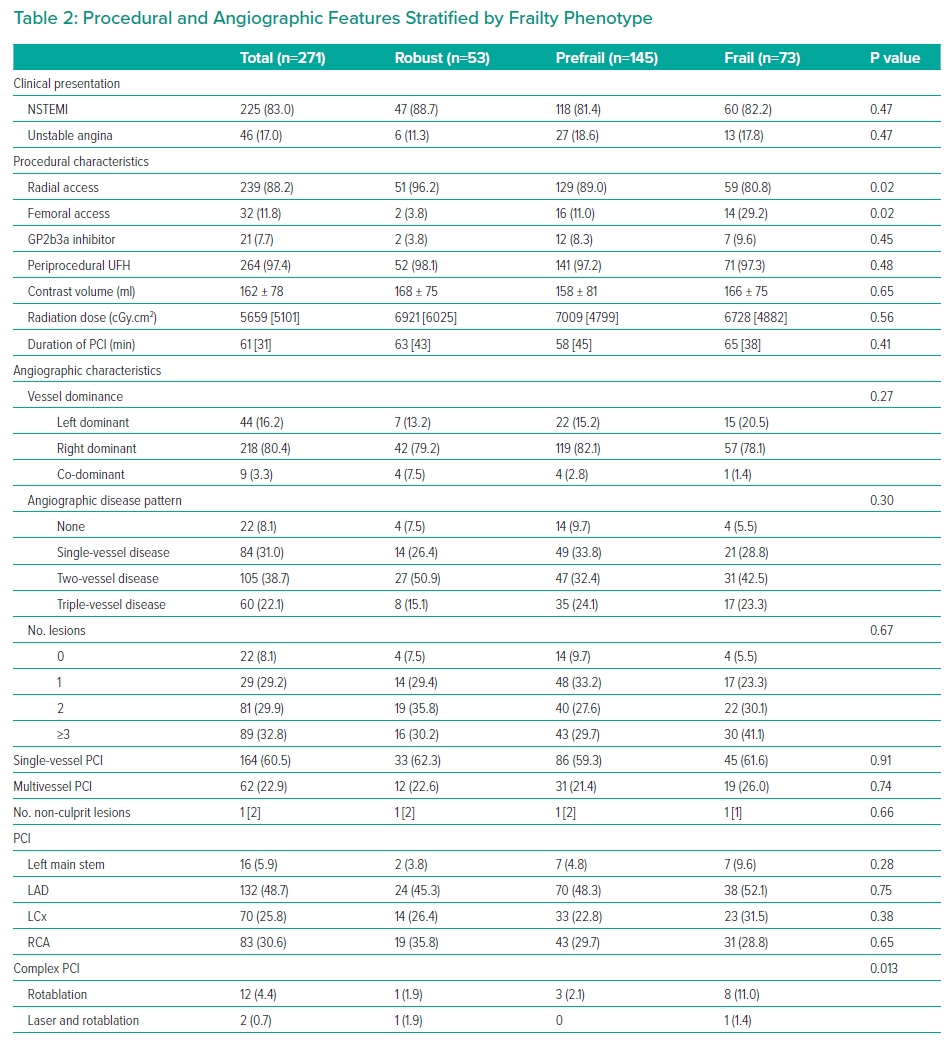
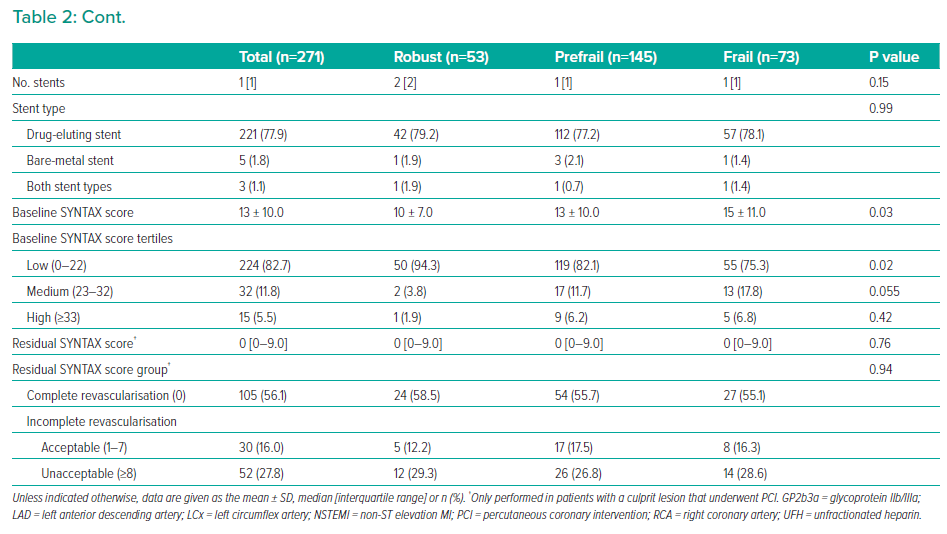
Vascular access via the femoral (as opposed to radial) artery was less common in robust than prefrail and frail patients (n=2 [3.8%] versus n=16 [11%] and n=14 [29.2%], respectively; p=0.02). The mean SYNTAX score increased with increasing frailty (10 ± 7.0, 13 ± 10.0 and 15 ± 11.0 in the robust, prefrail and frail groups, respectively; p=0.03), indicating more complex coronary artery disease (Table 2).
Culprit Lesion Angiographic Analysis
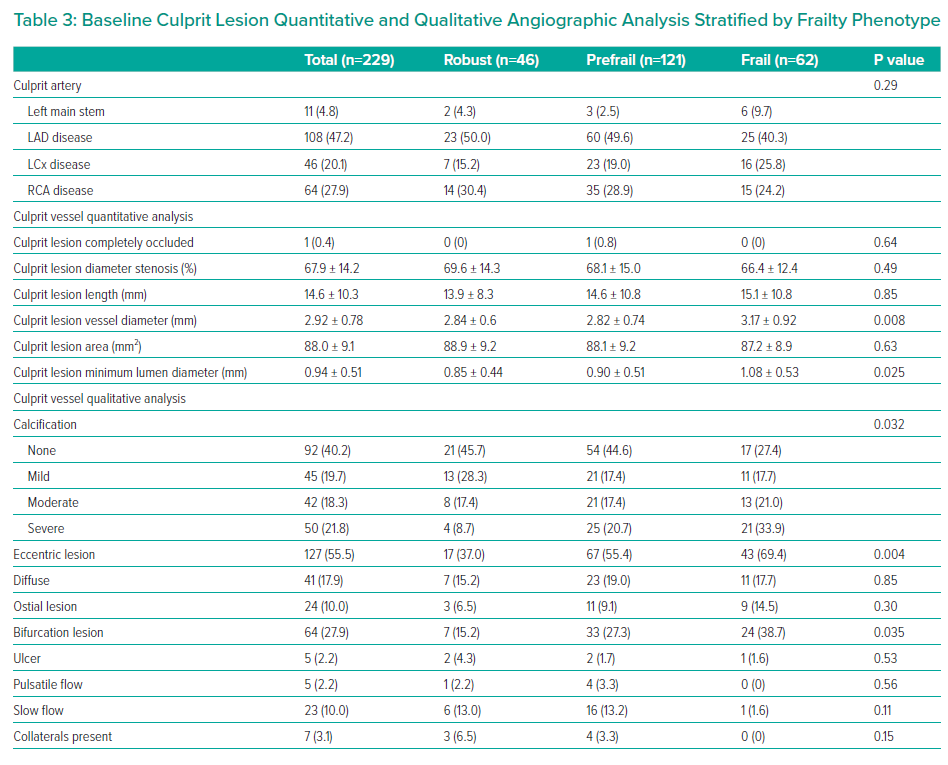
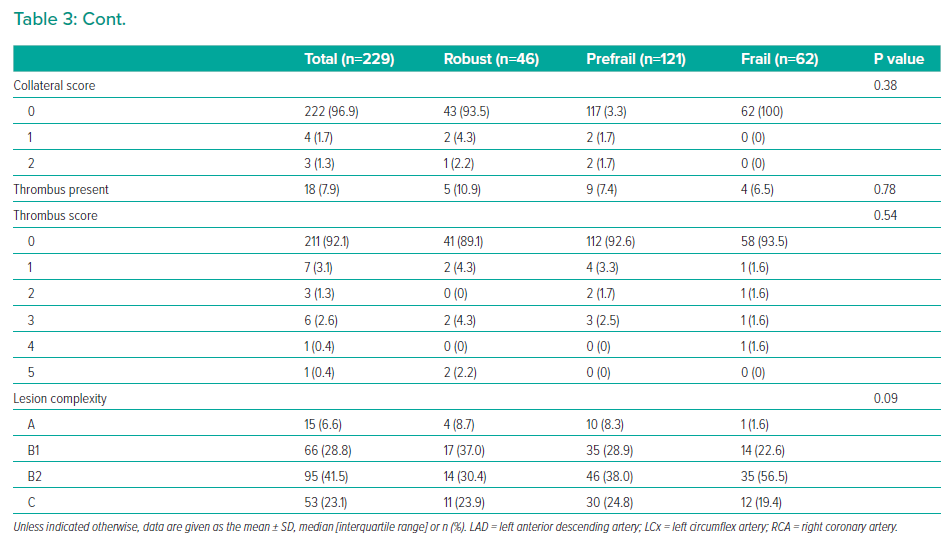
Of the 229 patients with culprit lesions, 211 (92.1%) had culprit lesion PCI performed. Robust patients had significantly smaller culprit lesion vessel diameter than prefrail and frail patients (2.84 ± 0.6 versus 2.82 ± 0.74 and 3.17 ± 0.92 mm, respectively; p=0.008), as well as significantly smaller culprit lesion minimum lumen diameter (0.85 ± 0.44 versus 0.90 ± 0.51 and 1.08 ± 0.53 mm, respectively; p=0.025) and a lower proportion of severe culprit lesion calcification (n=4 [8.7%] versus n=25 [20.7%] and n=21 [33.9%], respectively; p=0.032; Table 3). Frailty category was not associated with the likelihood of culprit lesion PCI being performed (n=42 [91.3%], n=110 [90.9%] and n=59 [95.2%] in the robust, prefrail and frail groups, respectively; p=0.58). There were no differences between frailty groups and post-PCI culprit lesion quantitative angiographic measurements (Supplementary Material Table 2).
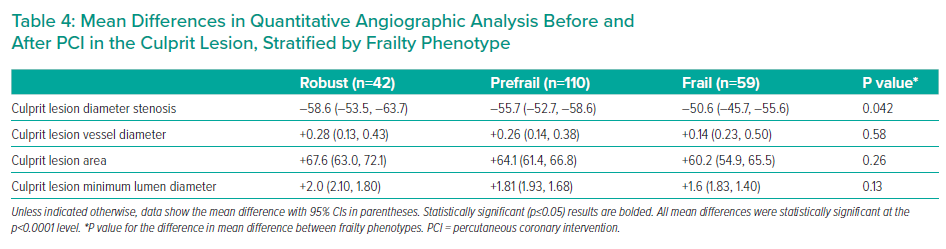
Improvements in mean culprit lesion diameter stenosis were significantly greater in robust patients (–58.6%; 95% CI [–53.5, –63.7]) than in prefrail (–55.7; 95% CI [–52.7, –58.6]) and frail (–50.6%; 95% CI [–45.7, –55.6]) patients (p=0.042; Table 4). Overall, there was a low periprocedural complication rate (n=12; 5.6%) with no significant difference between the robust, prefrail and frail groups (n=2 [4.8%], n=8 [7.3%] and n=2 [3.4%], respectively; p=0.56; Supplementary Material Table 3).
A residual SYNTAX score was calculated for 187 (81.7%) patients. The cohort median residual SYNTAX score was 0 (IQR 0–9.0), with 56% of the whole cohort having a residual SYNTAX score of 0. There was no significant difference in median residual SYNTAX score between frailty phenotypes, with all frailty groups having a median score of 0 (IQR 0–9.0; p=0.76; Table 2).
Multivariate Logistic Models of the Association Between Frailty and Angiographic Parameters
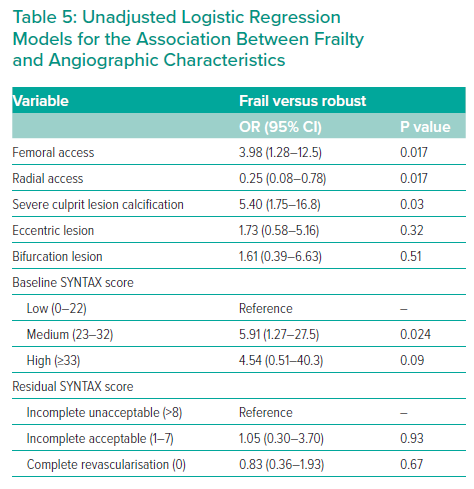
Frail patients had a greater than fivefold increase in the odds of severe culprit lesion calcification compared with robust patients (unadjusted OR 5.40; 95% CI [1.75–16.8]; p=0.03). In fully adjusted analyses, there was no association between frailty and a high (≥33) baseline SYNTAX score (adjusted OR 2.03; p=0.74) or frailty and a residual SYNTAX score of zero (adjusted OR 2.59; 95% CI [0.46–14.4]; p=0.27; Table 5 and Supplementary Material Table 4).
Clinical Outcomes at the 5-Year Follow-up
In all, 264 (97.4%) patients in the angiographic cohort completed the 5-year follow-up and are included in the exploratory cohort analysis. The median follow-up was 61.5 months. MACE occurred in 161 (60.9%) patients. For the whole cohort, a high (≥33) baseline SYNTAX score was associated with MACE in an unadjusted univariate analysis (HR 1.44; 95% CI [1.12–1.84]; p=0.004) and this association remained significant after adjustment for age and sex (HR 1.40; 95% CI [1.08–1.81]; p=0.01). A residual SYNTAX score ≥8 was associated with MACE in an unadjusted univariate analysis (HR 1.23; 95% CI [1.01–1.50]; p=0.037) and the association remained significant after adjustment for age and sex (HR 1.22; 95% CI [1.00–1.49]; p=0.047).
Discussion
In this prospective cohort study of older adults with NSTEACS, frail adults presenting with NSTEACS had more severe culprit lesion calcification, but this did not affect the likelihood of these patients receiving complete revascularisation. Both high baseline and residual SYNTAX scores were associated with adverse outcomes at 5 years.
International treatment guidelines increasingly recommend a patient-centred approach, with an assessment of frailty status when managing older adults with NSTEACS.11,12 Despite the fact that this cohort is increasingly a larger proportion of those presenting with NSTEACS, older patients are under-represented in clinical research, meaning evidence to guide decision-making is limited.3 This study presents the first analysis of the impact of the frailty phenotype on angiographic and procedural characteristics and their association on long-term adverse outcomes.
It has been previously hypothesised that the value of the SYNTAX score in predicting long-term adverse outcomes in the very oldest patients may be outweighed by other factors not yet defined.24 The data we present show that, independent of age, the frailest patients have a statistically significantly higher baseline SYNTAX score. However, further large-cohort studies are needed to determine the clinical significance of the 5-point difference in SYNTAX scores between frail and robust patients. The frailty phenotype may play an important and previously unmeasured role in the complexity of coronary artery disease found at the time of coronary angiography. Reverse causality is possible, with the presence of complex coronary artery disease contributing to the development of frailty through limitation in physical activity and subsequent slowness, both of which are criteria of the Fried frailty phenotype.17 In an exploratory analysis, there was an association between a high baseline SYNTAX score and the 5-year incidence of MACE. As the population ages and the prevalence of the frailty phenotype increases, clinical and angiographic scoring systems that remain accurate when applied to this cohort are important. The ongoing British Heart Foundation SENIOR-RITA trial (NCT03052036) is a large (n=1600) randomised trial investigating the role of invasive management in all-comer frail, older adults with NSTEACS. The analysis will include a preplanned subgroup analysis by frailty phenotype in addition to qualitative and quantitative angiographic analyses of participant angiograms, which will provide data on angiographic and procedural characteristics and clinical outcomes in a randomised control trial setting.

{kind=link}
Frail adults had more than fivefold increased odds of severe culprit lesion calcification compared with non-frail patients. Frail patients also were more likely to require complex PCI, likely as a consequence of increased culprit calcification. Although vessel calcification is an established age-dependent process, the age-independent association with frailty is a novel finding.25 The underlying pathophysiological processes are unclear; however, inflammation is considered a key process in atherosclerosis, in addition to coronary artery calcification, and is increasingly considered as key in the pathogenesis of the frailty phenotype.25–27 In a previously published analysis of the ICON1 study cohort, non-robust patients had a greater presence of high-risk lesions on virtual history intravascular ultrasound imaging, with a 2.81 increased adjusted odds (95% CI [1.06–7.48]; p=0.039) of the presence of thin cap fibroatheroma, independent of age.28 It is increasingly clear that frail adults presenting with non-ST segment elevation MI have more procedurally challenging angiographic characteristics, independent of age.
In a recently published long-term follow-up analysis of the ICON1 study cohort, frail patients had a significantly adjusted increased hazard of incidence of the primary composite outcome compared with robust patients (HR 1.81; 95% CI [1.00–3.27]; p=0.048), with similar findings for adults in the ICON1 study cohort with a higher burden of multimorbidity.29,30 Further work is needed to investigate the effects of the angiographic characteristics on outcomes in these frail, multimorbid patients in the context of large, well-powered studies allowing granular analysis.
Notably, 22 (8.1%) patients, 4 (5.5%) of whom were frail, had no culprit lesion identified and therefore are classified as MI with non-obstructive coronary arteries (MINOCA). This is a novel finding of the rate of MINOCA in this older, frail age group with NSTEACS. This presentation of ischaemia may be contributed to epicardial vasospasm and coronary microvascular dysfunction, but further research is needed, particularly in older adults.31
The risk–benefit ratio of coronary intervention in these patients is unclear and interventional cardiologists, therefore, need to be selective when undertaking PCI. Despite frail patients having a high SYNTAX score at baseline, with an associated higher likelihood of complex coronary artery disease, this did not affect procedural complications, which were similar between frailty phenotypes. In addition, after PCI was performed, residual SYNTAX scores were similar between frailty groups. The residual SYNTAX score has been shown to predict 5-year mortality following PCI; therefore, these findings may suggest that despite an initially adverse angiographic profile and a more challenging procedure for the operator, the operators achieved complete revascularisation equally in all patients, regardless of their frailty status.23 In our exploratory analysis, a higher residual SYNTAX score was associated with MACE after 5 years, but it is important to note that this analysis was not formally powered.
There are some limitations to this study. This study recruited patients that had already been referred for coronary angiography; therefore, the very oldest and frailest patients may have been excluded at the referring hospitals. A large limitation of this study is the small number of patients, particularly at the extremes of Fried frailty (i.e. in the robust and frail groups). Consequently, the CIs for the OR of certain angiographic characteristics (particularly calcification) are very wide. The overall SYNTAX score for the cohort is also low. Despite this, frail older patients are difficult to recruit to clinical trials in cardiology, and these findings should be considered hypothesis-generating. Further detailed angiographic analysis in a large cohort of older patients is preplanned in the ongoing British Heart Foundation SENIOR-RITA Trial.
In conclusion, frail adults presenting with NSTEACS have more severe baseline coronary artery calcification than robust adults, independent of age. Frail adults were just as likely as robust patients to receive complete revascularisation. In an exploratory analysis, baseline and residual SYNTAX scores were associated with MACE at 5 years.
Click here to view Supplementary Material.
Clinical Perspective
- Frail patients have more adverse angiographic characteristics than robust adults, particularly severe culprit lesion calcification, independent of age.
- Despite more complex coronary artery disease, frail patients are just as likely as robust patients to receive successful complete revascularisation.
- In exploratory analysis, baseline and residual SYNTAX scores in older frail adults referred for invasive treatment for NSTEACS were associated with MACE at 5 years.