An arteriovenous fistula (AVF) is an abnormal communication between an artery and a vein, resulting in pressurisation of the venous circulation and increases in size and flow of both vessel systems. AVFs have an important therapeutic use in haemodialysis access, but can also be pathologic. Here, we present the case of an uncommonly large and chronic AVF in the popliteal fossa, probably secondary to previous knee surgery.
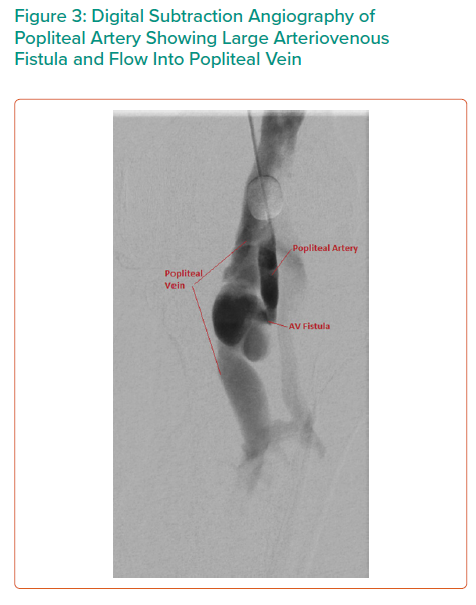
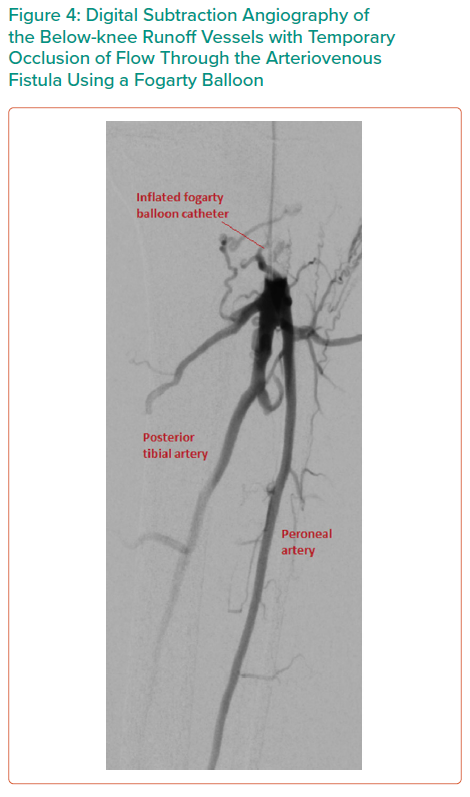
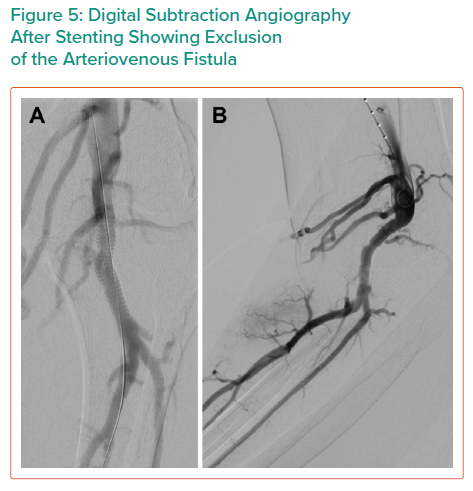
A 40-year-old man presented with years of progressive leg swelling and venous varicosities. Lower limb computed tomography angiography and subsequent digital subtraction angiography demonstrated a large popliteal arteriovenous fistula (AVF). This was treated successfully by endovascular technique with a Viabahn stent (WL Gore) in the popliteal artery to exclude the AVF. AVFs of this size and chronicity are rare, and this case demonstrates a successful endovascular method of treatment.
AVFs of the lower extremity are uncommon, particularly of the size and chronicity reported here. Causes are primarily traumatic or iatrogenic, but spontaneous cases due to aneurysmal dilation from Marfan disease, human immunodeficiency virus arteritis, and unknown causes have also been reported. Complications without repair may include symptoms of venous congestion with subsequent venous ulceration, venous thromboembolism, arterial steal, and high-output cardiac failure.
Surgical options include open surgical repair, endovascular repair, and a combination of open surgery and endovascular techniques. It was the authors’ opinion to undertake endovascular repair because of the large and multiple arterialised varicosities in the popliteal fossa. Endovascular options include covered stent, coil embolisation, and insertion of vascular plugs. It was the authors’ preferred option to proceed to covered stent alone because of the anatomic configuration in this case.