Background: Giant abdominal aortic aneurysm (GAAA) is defined as aortic diameter >100 mm – a rare variant amongst the acute aortic syndromes. Detection of new abdominal aortic aneurysms (AAAs), or those enlarging, is not uncommon; however, it is unusual to find those bigger than 70 mm and remain asymptomatic. Here, we report the subtle presentation of a 130 mm GAAA, and the radiographic features of impending rupture.
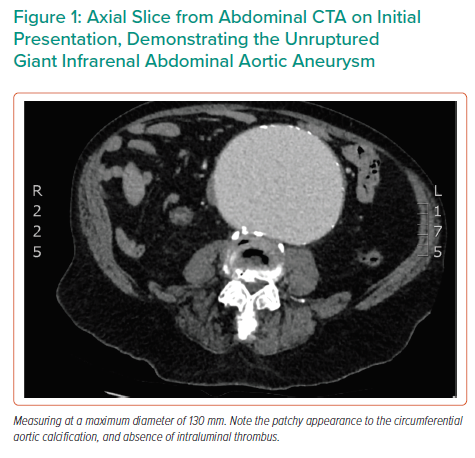
Case report: An 83-year-old man presented to hospital with intractable nausea. He was highly comorbid and frail, but otherwise was haemodynamically stable and pain-free. Abdominal examination revealed a large, non-tender, pulsatile mass, confirmed to be a AAA by bedside ultrasound. CT angiogram (CTA) was undertaken, demonstrating a 130 mm infrarenal GAAA, with patchy circumferential atherosclerosis and no aortic thrombus burden (Figure 1). Given personal wishes, the patient opted for conservative antiemetic management and discharged home.
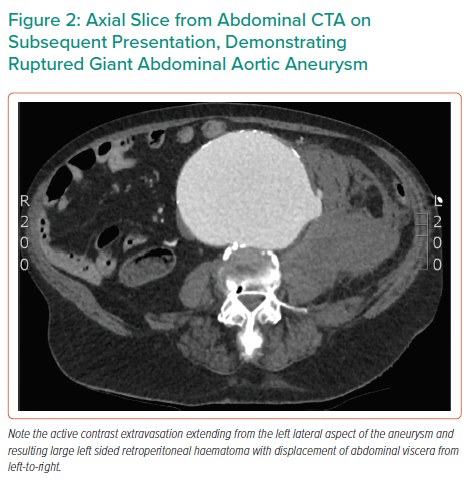
The following day he presented via ambulance to the Emergency Department, profoundly shocked. Resuscitation measures provided a short period of stability, allowing for a repeat CTA. This demonstrated the GAAA had ruptured, with a large left-sided retroperitoneal haematoma displacing the abdominal viscera entirely, with surrounding fat-stranding and free-fluid (Figure 2). As per his wishes, he passed away later that day.
Discussion: Medical imaging is key in decoding the urgency of a suspected unruptured AAA. Ultrasound provides rapid estimation of aortic diameter (greatest predictor of rupture); however, outside of a dedicated vascular laboratory this is limited in identifying other nuances of impending rupture. CTA is the gold-standard in AAA evaluation. Circumferential aortic calcification is important, notably checking for discontinuations, which may represent aortic wall weakness and potential future rupture sites. Luminal thrombus is a significant finding, where aortic-wall-stress studies have found increasing thrombus-rind to be protective against rupture. Contrast enhancement dissecting through aortic-thrombus is known as the hyperattenuating crescent sign, an early and specific feature of impending rupture.