









The PROTECT-Kidney trial was designed to address the important clinical issue of contrast-induced acute kidney injury (CI-AKI), which was shown to be associated with higher mortality in patients after percutaneous coronary intervention (PCI).1 CI-AKI ranks second among all causes of acute kidney injury (AKI) and contributes to inappropriately low rates of coronary angiography in patients with chronic kidney disease.2,3 There is a tendency for higher-risk patients to receive more conservative therapy for cardiovascular diseases, even though it has been shown that undergoing coronary angiography can reduce the risk of death by half for patients with chronic kidney disease from diseases such as non-ST-elevation MI and acute coronary syndrome.3 A study performed in 2019 found that the incidence of AKI during Impella-supported high-risk PCI in patients was lower than the predicted rates of AKI.4 These data led to the need for a prospective randomised trial to further explore the protective strategy of the Impella to prevent AKI during high-risk PCI.
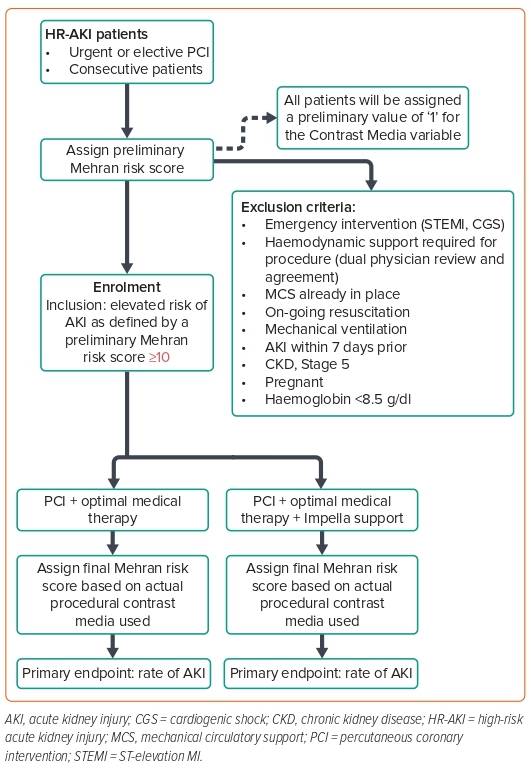
The PROTECT-Kidney pilot trial is a prospective randomised study investigating the role of Impella to maintain kidney function in a high-risk cohort for CI-AKI. The Mehran score was used to quantify the risk of AKI after contrast administration and patients with a Mehran score of ≥10 were included in the trial.5 The incidence of CI-AKI was detected by serum creatinine concentrations, and MRI was used to assess kidney function. The PROTECT-Kidney pilot trial was designed with a sample size of 40 to assess safety and feasibility, and the PROTECT-Kidney trial was powered at n=200 to detect efficacy on CI-AKI. Patients in both the Impella and control arms underwent MRI before and after coronary angiography. The primary endpoint was the incidence of CI-AKI, as defined by the Acute Kidney Injury Network’s (AKIN) definition: an increase in creatinine ≥0.3 mg/dl from baseline within 48 h after the procedure (Figure 1).
Dr Westenfeld presented the preliminary results from the PROTECT-Kidney pilot trial. With 30 patients enrolled thus far, the mean (±SD)Mehran score was 13.0 ± 2.9 in both the Impella and control arms and there was an individual AKI risk of 27% in the Impella group, compared with 28% in the control group, predicted by the Mehran score. In the Impella and control groups, mean patient age was 77.0 ± 6.5 years and 78.0 ± 6.3 years, respectively, and 53% and 50% of patients, respectively, were on anticoagulation therapy. The Charlson Comorbidity Index-derived likelihood of 10-year survival was 15.0 ± 19.9 and 13.0 ± 23.6 in the Impella and control arms, respectively. Mean left ventricular (LV) ejection fraction was 41.0 ± 13.2% in the Impella group, compared with 48.0 ± 7.4% in the control group. Mean contrast volumes used were 140.0 ± 51.1 and 152.0 ± 59.5 ml in the Impella and control groups, respectively. The primary endpoint of AKI occurred in 43% of patients in the control group, compared with 20% in the Impella arm. Renal function remained unchanged after contrast administration for 14% of patients in the control arm, compared with 60% in the Impella arm. Based on these data, Dr Westenfeld predicted that if the trial is scaled up, the projected p-values for the primary endpoint will be significant for a sample size of 200.
Dr Westenfeld discussed the potential mechanisms of renal protection by Impella during high-risk PCI. From the haemodynamic and MRI data obtained from the pilot study, he showed that patients in the control arm experienced a rise in LV end-diastolic pressure after PCI, whereas patients in the Impella arm did not. Further, looking at the blood oxygenation level-dependent MRI measurement obtained before and after contrast use, patients in the control arm showed a heterogeneous but significant oxygenation drop of the renal medulla after contrast use, whereas oxygenation levels were largely preserved in patients in the Impella arm.
Dr Westenfeld summarised that the interim analysis of the PROTECT-Kidney trial revealed less AKI (n.s.) and a higher proportion of patients with unchanged kidney function following contrast administration (p<0.05) in the Impella high-risk PCI group compared with control. The treatment groups were well matched for kidney function and the risk of AKI, and exhibited a low abundance of severely reduced LV function, although both groups had considerable comorbidities, these were well-balanced. No safety concerns were detected in the pilot trial. Patients in the Impella arm were protected from an increase in LV end-diastolic pressure during catheterisation and displayed a trend for increased diastolic blood pressure along with stabilised oxygenation of the kidney medulla, which was verified by MRI. Dr Westenfeld concluded that he expects the PROTECT-Kidney trial to demonstrate the nephroprotective effect of Impella, and the results will help decipher the potential underlying pathophysiology.